June 4-
In contrast to governmental paralysis and confusion caused by the pandemic, pharmaceutical and biotech firms around the globe are swarming Covid-19 in an effort to stop it in its tracks.
Last September, Gallup released an opinion poll that surveyed Americans’ views of U.S. businesses, ranking 25 different sectors from very positive to very negative. The pharmaceutical industry came in dead last, lower than at any time since Gallup started the poll in 2001.
“We’re below Congress, below bankers, below tobacco,” lamented Ken Frazier, chief executive of drug giant Merck.
What a difference a global pandemic makes.
Today the world is depending upon the pharmaceutical industry to not only save lives, but economies around the world. At this very moment, pharmaceutical companies and biotech startups from San Francisco and Boston to Tianjin, Tokyo and Galilee, are staging a multi-front battle against the novel coronavirus akin to the sea, land and air assault conducted by the allies against Nazi Germany on D-Day during World War II.
There are no fewer than 267 different COVID-19 remedies in development, according to an analysis by Umer Raffat, a senior managing director of investment bank Evercore ISI, with more experimental treatments being added almost daily. This includes testing drugs already available but designed for other ailments, new experimental therapeutics, and vaccines that are being developed from scratch. [see Table of Top 50 below]
The attack against coronavirus is coming from all sides. There are synthetic peptide-based vaccines consisting of two or more linked amino acids created in a lab to immunize against the virus; there are so called nucleic acid vaccines genetically engineered from DNA or RNA sequences of the pathogen; antiviral medications, similar to Tamiflu, that target the virus itself; there are new remedies using existing arthritis drugs to contain the immune system, which sometimes inadvertently kills patients as it unleashes its force on COVID-19. Underlying the multitude of efforts underway is the reality that most drugs in development are ultimately unsuccessful.
“A lot of companies are doing the rational thing: testing therapies already in their pipeline which have a plausible mechanism of action. We need to get drugs into clinical trials rapidly so we can quickly learn and double down behind promising results and follow the winners,” says Vivek Ramaswamy, CEO of Roivant Sciences, a drug development firm that acquires hidden gems among forgotten drugs in the pharmaceutical pipelines.
“The idea is to find the best horse in each of the categories. Antivirals plus host immune response modulation makes a lot of sense, but we need to find the best therapeutic in each category, for the right patient population.” says Ramaswamy, who studied biology at Harvard, was a hedge fund analyst and earned a Yale law degree before he began building his innovative biotech firm in 2015. “For antivirals, is it a nucleoside, or an antimalarial which prevents viral propagation in a different way? For immune response modulation, is it anti-IL-6 or anti-GM-CSF? The answer may differ by patient population. Let’s sort those questions out quickly.”
Ramaswamy says that it’s difficult to have a national strategy for the coronavirus predicated on a vaccine that would provide immunity to COVID-19 because it will take a year to a year-and-a-half, optimistically, to have something ready for use on a national scale. But if latency occurs and the coronavirus becomes a perennial problem, akin to the seasonal flu, vaccines will be important.
Sanofi’s vaccine unit is partnering with the federal government’s Biomedical Advanced Research and Development Authority, piggybacking off work that was done on a SARS vaccine and its recombinant vaccine program. But Sanofi doesn’t expect trials in patients for about a year-and-a-half.
Johnson & Johnson has been working on COVID-19 vaccines since January. In late March it announced its Janssen unit would be pushing forward a candidate in a $1 billion partnership with the federal government with the goal of rapidly supplying more than one billion doses. J&J says its vaccine should be in human trials by September and that first batches could be used for front-line medical workers by early 2021.
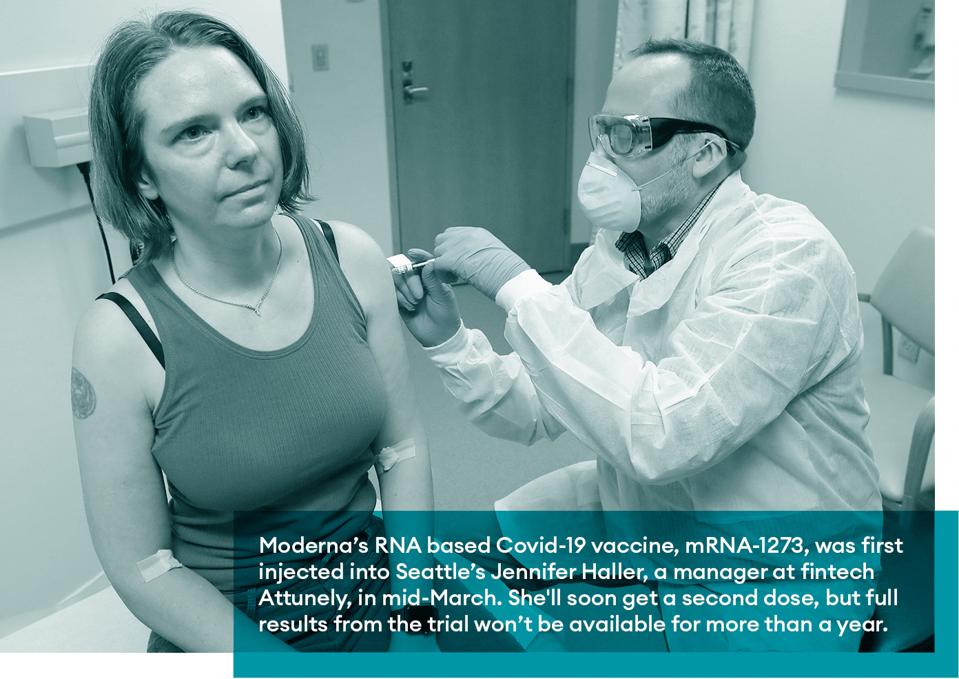
Cambridge, Massachusetts biotech Moderna Therapeutics also signed a partnership deal with the federal government’s BARDA. It claims that it may be able to shorten the relatively long development time for a vaccine. Like Ebola and measles, COVID-19 is an RNA virus, meaning it has no DNA but instead uses the host’s cells to replicate itself. Moderna specializes in developing drugs based on RNA. In this case it is attempting to give messenger RNA the cellular machinery to make proteins that generate an immune response in the body, creating antibodies that could protect against the virus itself. By the middle of March, Moderna started testing its RNA-based vaccine in low doses in people in Seattle.
Moderna’s billionaire CEO Stephané Bancel says his company’s vaccine could be available to medical workers as early as this fall. In fact Bancel is so eager to speed up the process, and confident about Moderna’s vaccine, that the company is already dipping into corporate funds to gear up and prepare materials for later stage clinical trials even though it hasn’t cleared its first hurdle.
The issue with the messenger RNA approach is that it was initially designed to be used in much more targeted and small scale situations, like cancer and rare diseases, as opposed to infectious disease. In fact, an mRNA vaccine has never even been approved by the FDA. If Moderna’s vaccine is effective, manufacturing enough RNA to provide immunity for hundreds of millions could be a challenge. Still, Bancel insists that Moderna could produce millions of doses by the fall.
“We need to practice some measure of social distancing until we have vaccines,” says Peter Kolchinsky, cofounder of $4 billion biotech hedge fund RA Capital Management and author of The Great American Drug Deal: A New Prescription for Innovation and Affordable Medicines.
TED S. WARREN / AP
Kolchinsky doesn’t expect any large-scale vaccines until the first half of 2021, at earliest. As a result he thinks all establishments that rely on public gathering should remain closed until then — from restaurants and sporting events, to subways and maybe even schools. “We’ll know if any of the first wave of vaccines are working during the June to October 2020 window. We can make better predictions as we see that data roll out,” Kolchinksy says. He thinks the mRNA vaccine could become available by the end of 2020, but it will likely require multiple doses per patient, which could translate into hundreds of millions of doses needed per month. Says Kolchinksy, “I’m keeping an eye on vaccines that could take just one dose to work, which could be the case for J&J’s vaccine.”
Another important and perhaps more pressing front in the war against COVID-19 is therapeutics because they promise to have an immediate impact on people already afflicted by the influenza as well as tamp down the impact of an expected second wave of the pandemic. Former FDA Commissioner Scott Gottlieb is urging the federal government to set up robust partnerships with companies working on therapeutics, just as it has with the vaccine makers.
Kolchinsky says it’s too early to tell which of the many therapeutics being tested will work, but he expects drug combinations will emerge. He adds some drugs might start to be available by fall to treat the most serious cases and that doctors might alter the way available drugs, like antimalarial remedy chloroquine or hydroxychloroquine, are used as fresh data on their efficacy become available. Hydroxychloroquine is already being used in some hospitals in combination with antibiotic azithromycin, often used for bacterial infections like strep throat and bronchitis.
Kolchinsky says that the attention being given to the malarial drugs is warranted because the drugs have shown some efficacy in pre-clinical in-vitro work. So far the early studies in people have been mixed, but it appears they may work better if someone infected with Sars-CoV-2 receives it early in treatment, much the way Tamiflu is administered. The trouble is coronavirus can have mild symptoms often ignored initially until it suddenly gets much worse. Malarial drugs like hydroxychloroquine require a prescription, so by the time they are prescribed by a physician, their efficacy against COVID-19 could be diminished.
In Japan, Fujifilm Holding subsidiary Toyama Chemical’s antiviral favipiravir, also known as Avigan, is showing promise in reducing the severity and duration of COVID-19. In a limited test of patients from China, those treated with favipiravir, which was approved as an antiviral for use in Japan in 2014, tested negative for the virus after four days compared to the 11 days it took the control group to recover.
Gilead’s antiviral remdesivir has shown preclinical promise but it needs to be administered early and intravenously. The concern is that people infected with Sars-CoV-2 might get it too late in the cycle. Results from some of remdesivir’s clinical trials are expected as early as this month.
David Witzke, co-managing partner of Avidity Partners, a biotech and healthcare hedge fund firm, points to rheumatoid arthritis drugs that inhibit the pro-inflammatory protein known as cytokine IL-6 as being potentially promising for COVID-19 patients in later stages, often in ICU units and on ventilators.
These drugs could be effective in reducing the risk of a cytokine storm of the body’s immune system. Cytokines are molecules that signal cells to marshal an immune response. In some COVID-19 cases, particularly younger patients, the overzealous molecules actually cause the immune system to not only vanquish the virus but go on to attack organs like the lungs and liver, causing failures and ultimately death. Sanofi and Regeneron’s Kevzara are working on a therapeutic designed to prevent such cytokine storms.
“Anti-inflammatory drugs, the IL-6 antibodies, like Actemra at Roche and the products at Regeneron, seem to be helpful in patients when their lungs get full of inflammation,” says Witzke. “These are drugs on the market [today] so they are available and if they are helping these late stage patients that will be a benefit. We are more optimistic about those drugs.”
Another set of remedies known as JAK inhibitors reduce IL-6 antibodies, but also attack a whole host of other pro-inflammatory cytokines. Jakafi and barticinib are two arthritis drugs in development by Delaware biotech firm Incyte and pharmaceutical giant Eli Lilly that are now being studied. JAK inhibitors are riskier because they offer a broad attack, akin to firing a shotgun rather than a rifle, at the problem. But the JAK inhibitors could also diminish the risk of a cytokine storm. Data on JAK inhibitor effectiveness on COVID-19 should be available by summer. Roivant’s Gimsilumab targets another cytokine, GM-CSF, which has been identified as causing severe respiratory distress for COVID-19 patients in China who required intensive care.
Another hotbed for coronavirus cures are monoclonal antibodies, which are antibodies that bind to the spike proteins of COVID-19 and ultimately neutralize it. Monoclonal antibodies can be “cloned” from blood plasma and Regeneron is a leader in this effort. For the novel coronavirus it has cloned antibodies from the blood of mice, which have been infected and recovered from the disease. If Regeneron’s new treatment proves effective in clinical trials it could be available by the fall. This could be a game changer because monoclonal antibodies can be used both as a cure for infected patients, as well as a kind of vaccine for the general population.
Depending on the half-life of the monoclonal antibody, a person could have coverage for up to a month, which could be very useful for those with a family member who has come down with an infection. Regeneron, which is selecting two antibodies for its COVID-19 cocktail treatment, is following the playbook that worked for it against the Ebola epidemic in the Congo.
“Regeneron is one of the best protein engineering companies in the world and they have one or more monoclonal antibodies. What is very encouraging is the virus does not appear to be mutating at any great rate,” says Witzke.
Eli Lilly and San Francisco’s Vir Biotechnology, are also using monoclonal antibodies to create their cure but they are harvesting their antibodies from human patients who have survived COVID-19. Antibodies naturally produced against the virus are being engineered into a remedy that the companies hope to mass produce. Vir said in March that it has identified multiple human monoclonal antibody development candidates that effectively thwart the virus and anticipates that human trials could begin within three to five months.
In a way, Vir and Eli Lilly are putting a modern spin on treatment that has been around for more than a century—using plasma and its antibodies from patients who have recovered from a viral infection and giving it to patients infected with the virus. In fact using convalescent plasma for treatment was effective against diptheria in the 1890s and scarlet fever in the 1920s. What drug companies like Vir and Eli Lilly are doi
Courtesy: Forbes: https://www.forbes.com/sites/nathanvardi/2020/04/08/handicapping-the-most-promising-of-267-potential-coronavirus-cures/#5223b9c77f23

